We present a virtual reality (VR) framework for the analysis of whole human body surface area. Usual methods for determining the whole body surface area (WBSA) are based on well known formulae, characterized by large errors when the subject is obese, or belongs to certain subgroups. For these situations, we believe that a computer vision approach can overcome these problems and provide a better estimate of this important body indicator.
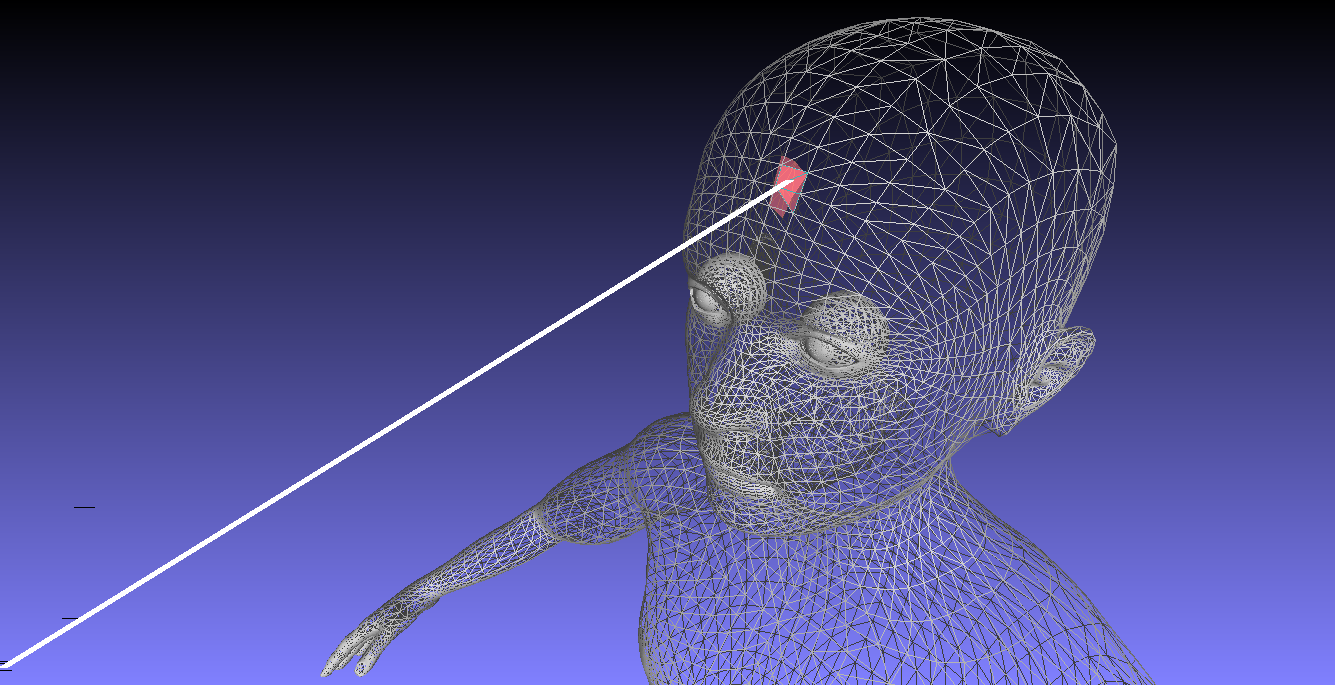
Unfortunately, using machine learning techniques to design a computer vision system able to provide a new body indicator that goes beyond the use of only body weight and height, entails a long and expensive data acquisition process. A more viable solution is to use a dataset composed of virtual subjects. Generating a virtual dataset allowed us to build a population with different characteristics (obese, underweight, age, gender). However, synthetic data might differ from a real scenario, typical of the physician’s clinic. For this reason we develop a new virtual environment to facilitate the analysis of human subjects in 3D. This framework can simulate the acquisition process of a real camera, making it easy to analyze and to create training data for machine learning algorithms. With this virtual environment, we can easily simulate the real setup of a clinic, where a subject is standing in front of a camera, or may assume a different pose with respect to the camera.
We use this newly designated environment to analyze the whole body surface area (WBSA). In particular, we show that we can obtain accurate WBSA estimations with just one view, virtually enabling the possibility to use inexpensive depth sensors (e.g., the Kinect) for large scale quantification of the WBSA from a single view 3D map.
Accurate determination of the whole body surface area (WBSA) is one topic that has been actively studied over the last century. From the initial estimate of Du Bois and Du Bois1 in $1916$ to recent work2, and despite many critiques3, the WBSA has attracted a lot of attention, driven primarily by the large variety of its applications.
The common methods for WBSA calculation are through some well known formulae. The most widely used formula for WBSA calculation is the one devised by Du Bois and Du Bois in $1916$. Moulds of plaster of Paris for 9 subjects were cut into small pieces in an attempt to measure the two-dimensional surface area of the skin. Each individual’s body/skin surface area was then calculated and Du Bois and Du Bois determined that WBSA was related to stature and weight by the formula: $0.007184 \times W^{0.425} \times H^{0.725}$, where W is the weight (in kg) and H is the stature (in cm) of the subject. Notably, this formula was derived from $9$ subjects only, one of whom was a child. Since the bodies of the subjects studied in the middle of the First World War are unlikely to be similar to the patients of the modern society, Mosteller4 proposed a new calculation of WBSA in $1987$. This formula is a modification of the WBSA equation by Gehan and George5.
Today there are many studies related to the verification of meaningful differences between WBSA measurements taken using a whole body three-dimensional (3D) scanner (criterion measure) and the estimates derived from each WBSA equation identified from systematic review6. The 3D scanners used are often cumbersome and slow, and have to be operated by specially trained personnel.
An alternative to the use of WBSA formulae is whole-body 3D scanning. There are three major issues with the 3D laser scanners: cost, speed, and physical space requirement. Classic 3D laser scanners use a laser beam to illuminate the surface. At the same time a receptor registers the beam distortion on the surface and computes the respective depth. The beam needs to cover all the space of the surface and it takes time to do so. This requires that the object be almost immobile and small movements can cause errors in the reconstruction. Modern laser scanners are fast enough to avoid this distortion, but still require a large room to contain the device.
The result of the scanning operation is usually ``raw’’ data in the form of a 3D $(x,y,z)$ point cloud. To reconstruct the mesh surface from the raw data, a surface reconstruction algorithm has to be applied. Without the face information it is not possible to relate the vertices to a face and thus compute the area of the surface. The 3D data, after surface reconstruction, is completed by other information than $(x,y,z)$ points. The reconstruction with triangles, for instance, fits many little triangles every $3$ points of the cloud. Then the calculation of the whole body surface area is reduced to a simple summation of the areas of all the triangles composing the mesh. This solution, unfortunately, is not as reliable and efficient as it looks. Key challenges in 3D body scanning include occluded areas, body parts registration, device complexity and portability. Yu et al.7 provide more detailed analysis on some of these problems.
Given these multiple problems, we decided to approach the WBSA calculation with an unusual methodology for this area. Our goal can be summarized with the following idea. Using a simple Kinect device we want to obtain the accurate WBSA calculation of any given person regardless of differences in gender, race, obesity, with the subject simply facing the device without the supervision of a trained personnel. We want to use just one device that can acquire only one view of the subject, simplifying the setting required for an accurate estimation, and making possible the accurate estimation in a home setting. The device will acquire just the visible portion of the body, and a subsequent prediction stage will reconstruct the overall WBSA.
Unfortunately, the described system needs training data to be reliable, representing a large number of body shapes with significant diversity. Since the collection of this large amount of data is expensive, time consuming, and very difficult, we decided to virtualize our training set, proposing a framework based on virtual subjects, computer vision and computer graphics techniques for the analysis and measurement of WBSA.
D. Du Bois, E. F. Du Bois, D. Du Bois, and E. F. Du Bois, “A formula to estimate the approximate surface area if height and weight be known,” Nutrition, vol. 5, no. 5, pp. 303–311, 1989. ↩
N. Jander et al., “Indexing aortic valve area by body surface area increases the prevalence of severe aortic stenosis,” Heart, vol. 100, no. 1, pp. 28–33, Jan. 2014. ↩
M. Sawyer and M. J. Ratain, “Body surface area as a determinant of pharmacokinetics and drug dosing,” Invest New Drugs, vol. 19, no. 2, pp. 171–177, May 2001. ↩
R. D. Mosteller, “Simplified Calculation of Body-Surface Area,” N. Engl. J. Med., vol. 317, no. 17, pp. 1098–1098, Oct. 1987. ↩
E. A. Gehan and S. L. George, “Estimation of human body surface area from height and weight.,” Cancer Chemother. reports, vol. 54, no. 4, pp. 225–35, Aug. 1970. ↩
N. Daniell, T. Olds, and G. Tomkinson, “Technical note: Criterion validity of whole body surface area equations: a comparison using 3D laser scanning.,” Am. J. Phys. Anthropol., vol. 148, no. 1, pp. 148–55, May 2012. ↩
C. Y. Yu, C. H. Lin, and Y. H. Yang, “Human body surface area database and estimation formula,” Burns, vol. 36, no. 5, pp. 616–629, 2010. ↩
 Marco Piccirilli
Marco Piccirilli